What is myasthenia gravis. Describe the biological basis of its treatment
Myasthenia Gravis (MG)
It is a potentially fatal autoimmune condition in which body develops T cell-mediated immunity against ACh receptors in the postsynaptic membrane in myoneural junction of the skeletal muscles.It is characterized by:
(i) Profound weakness of skeletal muscle
(ii) Impaired muscle contraction
(iii)Inability to maintain sustained contraction,
(iv) Early onset of fatigue.
It is due to defective transmission of impulse from nerve fibre to muscle fibre.
Pathophysiology
1. Formation of circulating antibodies to acetylcholine receptors – The antibodies developed against the receptors of the end plate bind to them and prevent uptake of ACh by the receptor.
The ligand gated Na+ channels fails to open and impulse cannot be generated.
Antibodies also destroy the receptors.
2. As a result, the number of ACh receptors on the motor end plate is decreased to 20% of the normal.
3. The subneural clefts also become smaller and flattened.
This decreases the surface area.
4. So, the effect of ACh on the end plate becomes less.
5.Thus, muscles cannot contract.
Note: Thymus appears to have a role in genesis of myasthenia as it is associated with enlarged thymus in most of the patients.
It appears it has role in the production of antibodies against Ach receptors.
Thymectomy improves the condition.
Clinical Features
• Myasthenia gravis affects females more.
•Extreme skeletal muscle weakness. The muscle strength is greatest in the morning and least in the evening.
• Initially eye ,facial, oesophageal and pharyngeal muscles are involved. The subject may develop diplopia (double vision), ptosis(drooping of eyelid) and toneless voice (husky voice).
Difficulty in chewing and swallowing are present.
toneless voice
3. The weakness spreads to other muscles slowly.
4.Involvement of respiratory muscles may lead to death of the subject.
Treatment
Management
#1 Medical
Principle:
• Ach levels should be increased at the motor endplate to dislodge the antibodies
• Antibody concentration in the blood should be reduced
a)Anticholine exterases:
•Neostigmine
•Ambenonium
•Endrphonium
These destroy ACh esterase and increase ACh concentrational neuromuscular junction. Hence, they are used in the treatment of myasthenia gravis.
b) Immunosuppreside agents: Glucocorticoids and azathioprine are immunosuppressive agents given to reduce the antibody titre as they destroy the lymphocytes
#2 Surgical: In some of the cases ,thymus is enlarged. In these cases, thymectomy improves the condition due to decreased production of ‘T’ cells .
Splenectomy is also indicated as if leads to a reduction in the production of immunocompetent cells.
Plasmapheresis:- This is done to remove the autoantibodies from plasma
Sequence of events of neuromuscular junction
Definition:
This is a functional union between the nerve terminal and a skeletal muscle fibre without anatomical continuity.
Note: each muscle fibre has one junction but occasionally has two junctions.
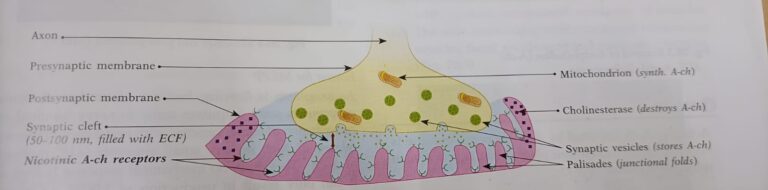
Events that Take Place During Transmission of Impulse Across NMJ(Neuro-muscular junction)
1. Arrival of impulse at the terminal end of the nerve fibre.
2.Depolarization of the synaptic knob.
3.Opening of voltage- gated Ca++ channels
4.Ca++ ions enter the synaptic knob
5.Vesicles move towards the active zones ( sites of vesicular rupture and release of the neurotransmitter. These are present just above the sub neural clefts)
6.Vesicles attach to the membrane of the synaptic knob.
7.Rupture of vesicles takes place and ACh is liberated into the synaptic cleft . About 200 vesicles rupture and each vesicle releases about 10,000 molecules of Acetylcholine.
8.Acetylcholine combines with receptors present on the motor end plate
9.Ligand-gated sodium and potassium channels on the end plate open.
10. Na+ enters the cell. K+ leaves the cell.
11. Development of end plate potential (EPP)
•Due to opening of the ligand-gated channels in the endplate membrane, a large number of Na+ ions enter the muscle fibre from the ECF.
•Few K+ ions move out. This causes a drop in the negativity of membrane potential from -90 to – 50mV. This is refferred to as endoplate potential. The endplate potential is a local potential, non-propogated, does not obey all-oreno wand decays exponentially.
12.Development of action potential on the sacrcolemma
•When EPP reaches the threshold (-50mV), it triggers opening of voltage-gated Na+ channels of the sarcolemma causing its depolarization.
•Action potential develops on sarcolemma due to opening channels of voltage – gated Na+ channels.
•Action potential is conducted throughout the length of the muscle fibre.
•This excitation process gets coupled with contraction , Ca++ is responsible for this coupling.
13.Removal of acetylcholine
The released acetylcholine is removed immediately by two ways:
•Most of the acetylecholine is destroyed by the enzyme acetylcholinestrase present in the basal lamina. Acetate and choline that are formed enter the terminal knob and participate in the synthesis of ACh.
•A small amount of acetylcholine diffuses away from the synaptic cleft.
•A small amount of ACh is taken back by the nerve terminal by reuptake phenomenon.
14. Removal of ACh at NMJ is essential for further conduction and relaxation of the muscle following contraction.
Note: If the nerve stimulus is repetative for several minutes, then it diminishes acetylcholine vesicle. This is called fatigue of neuromuscular junction