write down the function of thalamus
Relay station: The thalamus acts as a relay station for sensory information, receiving inputs from all major sensory systems (except olfaction) and relaying them to the appropriate cortical areas for further processing.
Sensory processing: The thalamus is involved in processing and integrating sensory information, such as touch, temperature, pain, vision, and hearing.
Motor control: The thalamus is also involved in motor control, specifically in regulating voluntary movements and coordinating motor activity.
Consciousness and attention: The thalamus plays a key role in consciousness and attention, as it is involved in regulating arousal and alertness.
Memory and learning: The thalamus is involved in memory and learning processes, particularly in the consolidation of long-term memory.
Emotion: The thalamus is involved in processing emotional information and plays a role in emotional regulation.
Sleep and wakefulness: The thalamus is involved in regulating the sleep-wake cycle and is thought to play a role in promoting sleep.
write down the function of hypothalamus
1. Regulation of body temperature
2. Regulation of activity of the anterior pituitary gland
3. Formation of the posterior pituitary hormones and the regulation of their secretion
4. Control of circadian rhythm 5. Control of sleep-waking cycle
6. Control of integration of the ANS 7. Control of hunger and feeding
8. Control of water intake and the sensation of thirst
9. Control of emotional behaviour
10. Integrated control of the CVS.
write down the function of basal ganglia
- Motor control: The basal ganglia play a key role in regulating voluntary motor movements and motor planning.
- Procedural learning: The basal ganglia are involved in procedural learning, which refers to the acquisition of skills and habits through repetition and practice.
- Cognitive functions: The basal ganglia are also involved in cognitive functions such as attention, working memory, and decision-making.
- Emotion and motivation: The basal ganglia are involved in processing emotional information and are thought to play a role in regulating motivation and reward-based behavior.
- Dopamine regulation: The basal ganglia receive input from dopamine-producing neurons and are involved in regulating the release of dopamine in the brain.
write down the function of cerebellum
- Motor coordination: The cerebellum plays a crucial role in the coordination and smooth execution of voluntary movements, including posture, balance, and fine motor skills.
- Motor learning: The cerebellum is involved in the acquisition and retention of motor skills and procedural learning.
- Sensory integration: The cerebellum receives input from sensory systems and integrates this information to aid in motor control.
- Cognitive functions: The cerebellum has also been implicated in cognitive functions such as attention, language processing, and working memory.
- Timing and rhythm: The cerebellum is involved in timing and rhythm control, including the timing of movements and the perception of time intervals.
- Emotional processing: The cerebellum is also involved in emotional processing, including the regulation of fear and anxiety.
- Disorders: Dysfunction of the cerebellum can lead to a range of motor and cognitive deficits, including ataxia, dysmetria, and dysarthria.
write down the function of dorsal column of spinal cord
1 Conscious proprioception – joint position and movement
2 Some unconscious exteroception and proprioception to the cerebellum via external arcuate fibers
3 Vibration sensation
4 Light touch (tactile sensation)
5 Tactile discrimination and localization
6. Stereognosis
7. Deep pressure with fine gradations
write down the features of brown sequard syndrome
- Paralysis on one side of the body, typically affecting the limbs and torso
- Loss of sensation on the opposite side of the body
- Loss of proprioception (the sense of body position and movement) on the same side as the paralysis
- An exaggerated reflex on the same side as the paralysis (spasticity)
- Loss of bladder and bowel control (incontinence)
- Sexual dysfunction
explain why REM sleep is called paradoxial sleep
REM sleep is also called paradoxical sleep because the sleeping person is difficult to arouse despite having a desynchronized EEG that is characteristic of the alert, awake state.
Behavioral changes
- During this stage of sleep, the brain is highly active, similar to the level of activity during waking hours, yet the body is largely paralyzed.
- REM sleep is characterized by rapid eye movements, hence the name, along with rapid and irregular breathing and heart rate.
- Despite the high level of brain activity, the body’s muscles are relaxed, leading to a lack of movement and muscle tone, which is paradoxical in nature.
- REM sleep is the stage of sleep associated with vivid dreams, which can be intense and bizarre, yet the person remains largely unaware of their surroundings.
- During REM sleep, the body’s thermoregulation system is compromised, leading to a decreased ability to regulate body temperature, which is paradoxical given the high level of brain activity during this stage.

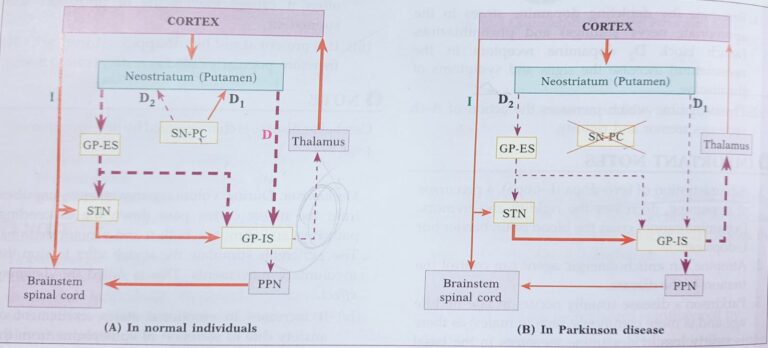
Parkinson's disease and its characteristics
It is also called paralysis agitans and is a depentive condition of the basal ganglia
- When the aetiology is ageing or idiopathic, it is called Parkinson’s disease. If associated with other intracranial causes or secondary to drugs, it is known as Parkinson’s syndrome or parkinsonism nigra.
- Its pathophysiology revolves around the basal ganglia.
- A variety of causes leads to degeneration of the basal ganglia. Oxidative stress due to ageing, genetic factors lead to formation of abnormal proteins (Lewy bodies, alpha synuclein) which cause damage to the cells of the substantia nigra and thus there is decrease in production of dopamine from these cells.
- There is loss of inhibition due to deficient dopamine.
- Thus, there is increase in inhibitory output to the external globus pallidus → decreased inhibitory output from the subthalamic nucleus → increased excitatory output to the internal segment of globus pallidus→ increased inhibitory output to thalamus → reduction in excitatory drive to the cerebral cortex.
Clinical Features:-
Akinesia/Bradykinesia
- -Lack of initiation of movements
- -retardation of movements
- -loss of automatic, associated movements (statue like appearance, mask like face)
- -Defect in speech
- -loss of timing & scaling of movements (micrographia)
Rigidity
- Hypertonia in the agonistic and antagonistic muscle
- Caused by increased discharge of gamma motor neuron
- 2 types of rigidity
- Cog wheel-intermittent resistance in passive movement
- Lead pipe-continuous resistance to passive movement
Tremor
- Occurs at rest
- Pill rolling tremor Alternate contraction & relaxation of agonists and antagonist of hands and finger
- frequency of 6-8 hertz/second
- Absent in sleep
Festinant gait
- body is bent forward
- moves forward with short quick shuffling steps as if to catch center of gravity
TREATMENT
Levo Dopa can cross the blood brain barrier, but dopamine cannot cross
write short note on lesion of cerebellum / cerebellar dysfunction?
They may be due to lesions in all the three parts of the cerebellum.
But the archicerebellum is rarely affected and so the disorders are due to either paleocerebellum or the neocerebellum or due to both.
Persons with chronic alcoholism, malnutrition or medulloblastoma develop either few or all symptoms.
Damage to the deep cerebellar nuclei or cutting of the red nucleus produces severe and lasting disturbances.
- Posture (attitude): The head rotated to normal side. Homolateral shoulder is lower than the other side. Weight is thrown on the normal leg. So, the trunk is bent with the concavity towards the affected side.
- Drunken gait: The person stands or walks on a wide base by spreading his feet and sways side to side. The person develops drunken gait. This is due to lesion in the vestibulocerebellum or vermis.
- Muscle tone: Decreased muscle tone is called atonia or hypotonia. This develops on the same side. The muscles become flabby and the limb swings like a flail. It is due to decreased facilitatory effect on the motor tracts. Hypotonia leads to asthenia.
- Reflexes: Deep reflexes become pendular, eg, knee jerk. – ankle jerk, etc whereas superficial reflexes are not affected. Pendular reflexes are due to a lesion in the spinocerebellum. In cerebellar lesion, the knee jerk exhibits several to and fro movements of the leg before it comes to rest, unlike a single movement of the leg in normal person.
- Voluntary movements: Lesions of the cerebellar hemi- spheres result in disturbances in beginning, coordination. terminating purposeful motor movements and rapid repro- gramming of opposite movements. The following features are present:
- Ataxia: Incoordinated movement is called ataxia. Motor ataxia is seen in cerebellar lesion.
(i) Asynergia Asynergia means lack of coordination between the agonists, antagonists and synergists that participate in a movement.
(ii) Decomposition of a movement: Loss of smooth transition of a movement from the proximal group muscles to the distal group. Movement occurs in stages.
(iii) Dysmetria: Failure to gauge the distance, direction, range and force of movement. The words hypermetria and hypometria are used to indicate overshooting or undershooting the target respectively.
- Intention tremor: This is the tremor that develops dur- ing movement. This develops due to a lesion either in the neocerebellum or in the intermediate zone. In other words, a defective planning or failure to correct the error during movement results in intention tremor. In a healthy person, error during movement is corrected in a single attempt. However, in cerebellar lesion, it takes several attempts to correct the error. Hence intention tremor appears at the end of a movement.
- Asthenia: Asthenia means weak movement and early onset of fatigue.
- Rebound phenomenon: It is due to the failure of the restraining effect following release of resistance suddenly.
- Dysdiadochokinesia: Inability to carry out rapid supination and pronation due to failure of rapid reprogramming of opposite movements.
- Nystagmus: The alternation of slow movement with fast return of the eyeball is called nystagmus, named according to the direction of the quick phase. This may develop due to lesion in vermis or flocculonodular lobe.
- Scanning speech: A person fails to pronounce lengthy word at a stretch. Instead he breaks a number of syllables. This is due to lesion of vermis
- Astasia : Unsteady voluntary movement is referred to as astasia.
1. Chartoid’s triad
2. Luclani’s triad (AAA)
a) Asthenia
b) Atonia
c) Ataxia
3. LPR’s tetrad (DDDD)
a) Dysmetria
b) Decomposition
c) Drunken gait
d) Dysdiadochokinesia
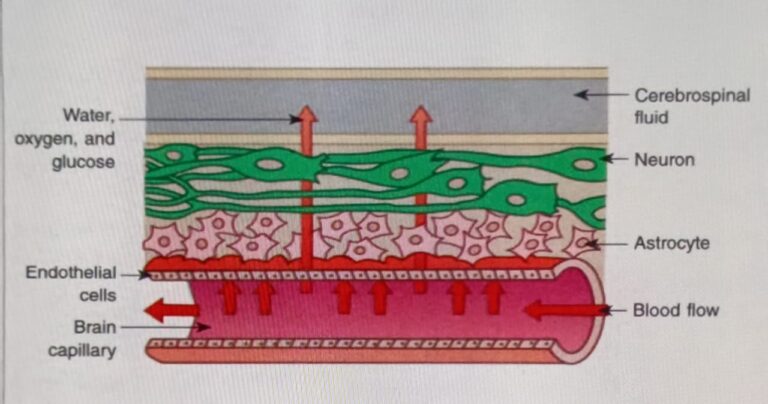
write short note on blood brain barrier
The term applies to the barrier between blood and the brain tissue. In fact this barrier exists at two places within the brain.
(1) One located at the choroid plexus and CSF fluid interface. Some physiologists use separate term for this as blood-CSF barrier (choroid plexus is slowly permeable to small ions and lipid insoluble substances and is impermeable to large lipid-insoluble compounds); and
(2) Other is located between the CSF and brain capillaries elsewhere than the choroid plexuses (true blood brain barrier). However, both the barriers are similar and the blood brain barrier (BBB) is the most common term used to refer to the net exchange of substance between blood and the brain.
There is an H+ gradient between brain ECF and blood; the pH of brain ECF is 7.33; whereas that of blood is 7.4.
In general rapidity with which substances penetrate brain tissue is inversely related to molecular size of substance and directly to lipid solubility of substance, thus water soluble polar compounds generally cross. slowly.
Therefore, these barriers are:
(i) Highly permeable to: water, O2, CO₂, sulpha drugs and erythromycin.
(ii) Slightly permeable to electrolytes: H+, Na+, K+, Mg2+, CH, HCO, and HPO42- glucose and some drugs e.g. penicillin, chloromycetin, tetracyclin.
(iii) Almost impermeable to: arsenic, gold, sulphur; urea; catecholamines; proteins and bile salts.
Development of BBB
BBB develops during early years of life, at this time cerebral capillaries are much more permeable than adulthood. Therefore, in severely jaundiced infants, bile pigments penetrate into nervous system and, in the presence of asphyxia, damage the basal ganglia (kernicterus) . However, this is not true in jaundiced adults.
Functions of BBB
(1) BBB protects the sensitivity of the cortical neurons to ionic changes with fluid bathing them. This helps to maintain constancy of environment i.e. concentration of K+, Ca2+, Mg2+, H and other ions in the CNS;
(2) It protects the brain from endogenous and exogenous toxins in the blood
(3) It prevents the escape of neurotransmitters into the general circulation.
Clinical Importance of BBB
1. Selection of drugs during management of meningitis: Sulpha and erythromycin are most commonly given to treat meningitis which can easily cross the BBB.
2. BBB breaks down in the areas of irradiation, infection or tumours, therefore, localization of pathological area with accuracy is possible with dyes or radioactive iodine labelled with albumin.
3. BBB also breaks down by sudden marked increase in B.P. or by I.V. administration of hypertonic fluids.